Article Text

Abstract
Objectives Individual metabolic characteristics and age-related changes may affect osteoarthritis (OA) risk as well as levels of potential OA biomarkers such as serum cartilage oligomeric protein (sCOMP) and urinary cross-linked C-telopeptide of type 2 collagen (uCTX2). We investigated hand OA and these putative OA biomarker characteristics at different ages in individuals with a propensity for healthy ageing, in controls, and in patients with OA.
Methods We investigated hand radiological OA (ROA) and levels of sCOMP and uCTX2 in the Leiden Longevity Study, which consisted of the middle-aged offspring of long-lived sibling pairs as metabolically healthy agers and their partners as controls, and for ROA we compared patients with OA at multiple joint sites from the Genetics, osteoARthritis and Progression Study with the healthy agers and controls.
Results Hand ROA mean scores were lower in the healthy agers than in controls. Lower hand ROA scores at higher ages were observed in healthy agers with low glucose levels. Furthermore, in healthy agers, a higher mean sCOMP level was observed than in controls. All study groups had higher sCOMP levels at higher chronological age. Likewise, uCTX2 levels were higher at higher chronological age in the controls and patients with OA, which was not observed in the healthy agers.
Conclusions Metabolic health in middle age is associated with less ROA and influences putative OA marker profiles, independently of chronological age. When used as OA biomarkers, it is relevant that independently of hand ROA status, uCTX2 is influenced by healthy metabolism and sCOMP is higher at higher chronological age.
- Hand Osteoarthritis
- Osteoarthritis
- Epidemiology
Statistics from Altmetric.com
Introduction
Osteoarthritis (OA) is one of the leading causes of disability and pain in the ageing population. Epidemiological studies have shown associations between OA and age, as well as between OA and unfavourable metabolic states (eg, high body mass index (BMI)) or metabolic disorders such as diabetes.1–3 Several mechanisms have been proposed to explain the deterioration in cartilage with age,4 but the link between age, metabolism and OA is not completely understood. The age-related component of OA may in part be ascribed to accumulated micro trauma, although there are large differences in age of onset of OA, which are not fully explained by accumulated lifetime joint use.5–7 Alternatively, intrinsic metabolic programming may affect OA risk, independently of mechanical stresses resulting from higher BMI in metabolic disorders. Inter-individual variation in metabolic programming may also influence the levels of potential biomarkers of OA such as serum cartilage oligomeric protein (sCOMP) and urinary cross-linked C-telopeptide of type 2 collagen (uCTX2).8 In the Genetics, osteoARthritis and Progression (GARP) Study, we have previously shown that uCTX2 levels reflect radiographic signs of OA (ROA) at joint sites across the whole body and that sCOMP, hand ROA and age cluster within a single heritable component.9 To attain the promise of the putative OA biomarkers, sCOMP and uCTX2, to be used for better classification of patients and assessment of disease progression rate, it is necessary to understand how age and metabolism affect their levels in the absence of, and in interaction with, OA. Such insights may come from studies focused on ageing and metabolism, independently of disease. The Leiden Longevity Study (LLS) consists of long-lived siblings, their middle-aged offspring and their partners as controls.10 When comparing these offspring, here referred to as healthy agers, with the controls, the familial longevity trait is reflected by a 30% increased survival, low prevalence of myocardial infarction and low prevalence of type 2 diabetes. Metabolic health, as defined by favourable parameters for serum lipid, glucose and insulin levels, is hypothesised to contribute to the survival benefit of the healthy agers.11 ,12
In this cross-sectional study design, we assessed the prevalence of hand ROA in healthy agers and controls and compared the levels of the potential OA biomarkers, sCOMP and uCTX2, at increasing ages in the two groups from the LLS and patients with OA from the GARP Study. This approach enables investigation of the behaviour of these potential OA biomarkers in association with age and metabolic health, independently of disease.
Materials and methods
The Leiden Longevity Study
Between 2002 and 2006, the LLS included 421 Caucasian families consisting of long-lived siblings with their offspring and the partners of their offspring. In this analysis, we included 329 healthy agers (from 225 unique families) and 329 partners (from 325 unique families) for which biochemical marker levels of sCOMP and uCTX2 were assessed in a follow-up visit between 2006 and 2008. Details of the LLS ascertainment are described in the online supplementary materials and methods.
The GARP Study
The ongoing GARP Study consists of 192 Caucasian sibling pairs of Dutch ancestry affected predominantly with familial symptomatic OA at multiple sites (two or more at the joint sites, hands, spine, hips and/or knees).13 Data on the levels of the biochemical markers, sCOMP and uCTX2, have been published previously and are available for 356 GARP patients.9 Details are described in the online supplementary materials and methods.
Hand ROA assessment
Hand ROA data for the GARP Study have been assessed previously.13 For the LLS, the hand radiographs were taken in the framework of a follow-up visit between 2009 and 2010 and scored according to the protocols used for the GARP Study (distal interphalangeal, proximal interphalangeal and carpometacarpal joints, Kellgren–Lawrence scores 2 or higher scored as OA, maximum score 20) by trained rheumatologists (MK and W-YK). Details are described in the online supplementary materials and methods.
Assessment of biochemical marker levels
To assess the LLS biochemical markers, the same procedures and assays were used in the same laboratory as was described previously for the GARP Study.9
Glucose levels were assessed in fasted baseline samples of the LLS collected between 2002 and 2006 and are described in detail in the online supplement and by Wijsman et al.11 Female healthy agers with glucose levels below the median and hand ROA data (N=57) were selected for analysis for hand ROA associations with age in the selected subgroup that shows evidence of the healthy ageing phenotype.11 ,10
Statistical analysis
χ2 statistics were used to test for significant differences between the fraction of male and female subjects in the study subgroups. Marker levels were logarithmically transformed and reported as such. The ages of men and women within each study subgroup were compared using a t test; tests for BMI differences between these groups were adjusted for age. For each gender-stratified study group, associations of biochemical marker levels with hand ROA were tested in a linear mixed model (LMM) in which family numbers were used as random factors to model robust standard errors and account for possible familial dependencies based on shared genetic or environmental factors.14–16 Tests for differences between the groups for the number of hand joints affected by ROA were corrected for age, sex, age×sex and BMI, or within each gender for age and BMI. Tests for mean differences in biochemical marker levels between healthy agers and controls were corrected for sex, age and sex×age, or within each gender for age alone. Because the patients with OA from the GARP Study and participants from the LLS were measured in different batches without overlapping samples, we did not compare the mean level of the biochemical markers between these studies. To test for changes in marker levels at different ages within each gender and within each study group, we applied a LMM analysis in which hand ROA was included as a covariate and family numbers were used as random factors to model robust standard errors and account for possible familial dependencies based on shared genetic or environmental factors.14–16 To test whether the increase in hand ROA, sCOMP or uCTX2 at consecutive ages in the controls, healthy agers and patients with OA were significantly different, we applied this LMM analysis including the additional interaction term age×study group. Further details of statistical analyses are provided in the online supplementary materials and methods.
Results
Study characteristics
table 1 shows baseline characteristics of the offspring of nonagenarian siblings (healthy agers) and their partners as controls. The characteristics of the patients with OA in the GARP Study are provided for comparison; the interactions of the markers with OA and age in the GARP Study have been published previously.9 Although the mean difference is relatively small, male controls and female healthy agers were significantly older in this study sample, because of the use of partners of the healthy agers as controls and the propensity of women to choose older partners (table 1). We therefore added an age×sex covariate to the analyses.
Study characteristics
Mean levels of hand ROA, sCOMP and uCTX2 in controls and healthy agers
We tested whether healthy agers are protected from OA by comparing hand ROA scores in healthy agers and controls. Table 2 lists the assessed mean number of hand joints with ROA out of 20 joints scored for the controls and the healthy agers.
Hand radiological osteoarthritis data for the Leiden Longevity Study
The mean number of ROA-affected hand joints was significantly higher in controls than in healthy agers (mean 3.10 vs 2.42, respectively, p=0.022). When we stratified for gender, we observed that the difference between female controls and healthy agers in the mean number of ROA-affected hand joints was significant (3.45 and 2.77, respectively, p=0.041). In men, the direction of effect was similar, but this was not significant.
To assess whether the mean differences in hand ROA were reflected by the potential OA biomarkers, uCTX2 and sCOMP, we measured mean OA biomarker levels in the healthy agers and controls (table 3).
Log-transformed levels of the biomarkers, sCOMP and uCTX2
In line with previous publications, for several study groups, we observed nominally significant associations of sCOMP and uCTX2 with ROA features (see online supplementary table S1). Fasting status did not significantly influence the levels of either marker (data not shown). In healthy agers, we observed a significantly higher mean sCOMP than in controls (mean sCOMP 0.99 and 0.97, respectively; age, sex and BMI adjusted p=0.018; table 3), which was mainly observed for women (mean sCOMP levels for healthy agers and controls 1.00 and 0.97, respectively; age and BMI adjusted p=0.025; table 3). When we tested whether the observed mean difference between healthy agers and controls for sCOMP levels and the number of hand joints with ROA was independent by applying a LMM including both variables as covariates, the number of hand joints with ROA remained significant (β=0.077, p=0.017), whereas sCOMP was not significant (β=−1.239; p=0.108), indicating that the differences in sCOMP levels may not be independent of hand ROA differences. No differences for mean uCTX2 levels were observed.
Age-related prevalence of hand ROA and marker levels in controls, healthy agers and patients with OA
Next, in the cross-sectional design, we investigated the association of hand ROA, sCOMP or uCTX2 levels with age in each study group, stratified for gender. Figure 1 shows scatterplots for the number of affected hand joints and age for all three study groups. In all study groups, we observed a higher number of ROA-affected hand joints at higher ages, which was most pronounced in women. The effect size of hand ROA versus age increased from female healthy agers (β=0.126, p=0.022) through controls (β=0.201, p<0.001) to GARP patients (β=0.240, p<0.001; figure 1). This increase in β between these groups was significant (analysis of variance: p<0.001, adjusted for BMI, groups coded 0, 1 and 2, respectively). In men, the number of ROA-affected hand joints increased slightly with age in all study groups (healthy agers, β=0.103, p=0.005; controls, β=0.086, p=0.039; GARP patients, β=0.061, p=0.516), but was significant only in the healthy agers and controls.
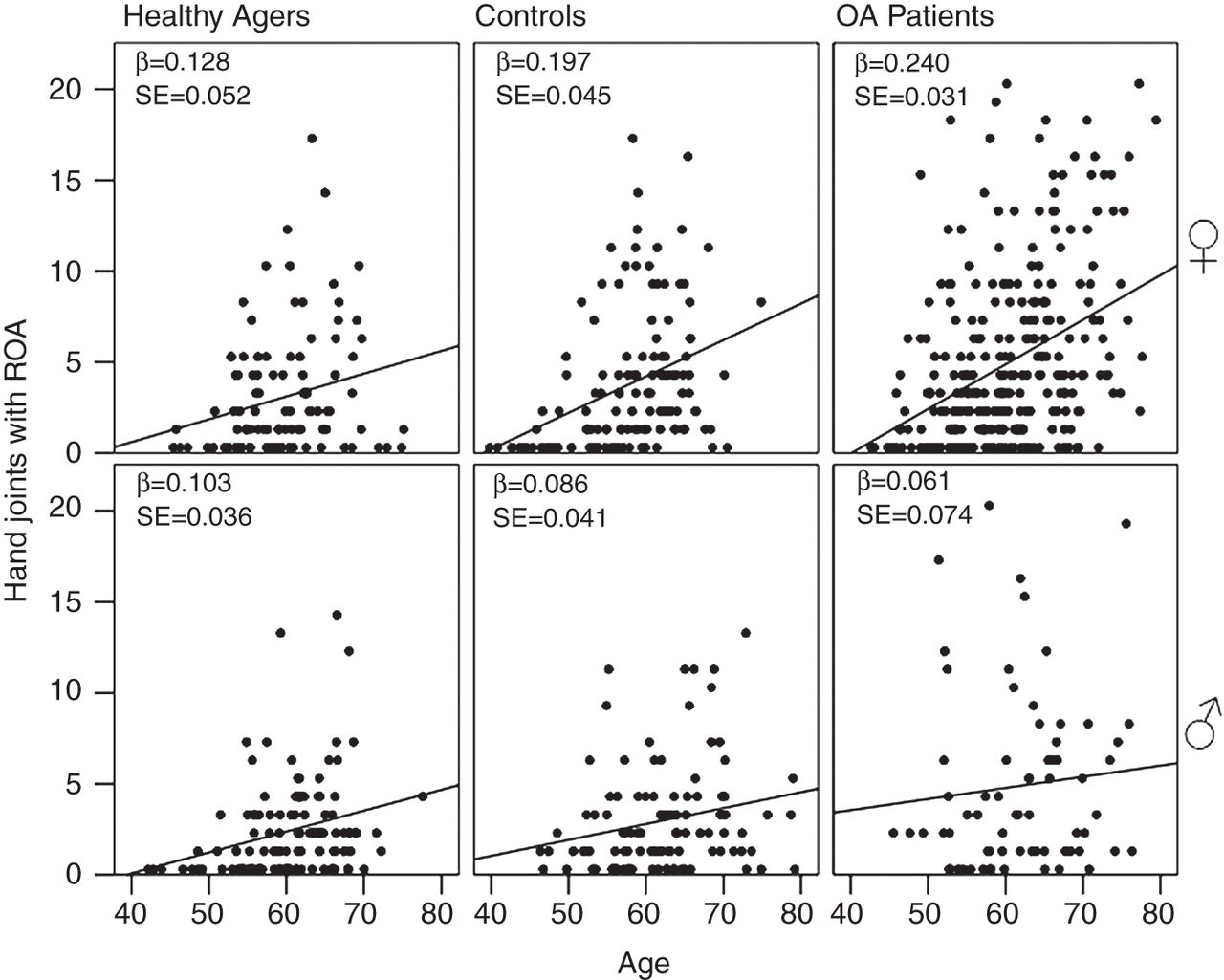
Scatterplots of number of hand joints affected with radiological osteoarthritis (ROA) against age, stratified by sex and study group: healthy agers (left), controls (middle) and patients with osteoarthritis (OA) (right). Top panes represent women, bottom panes represent men.β, unstandardised β estimate of regression adjusted for body mass index; SE, standard error of β estimate.
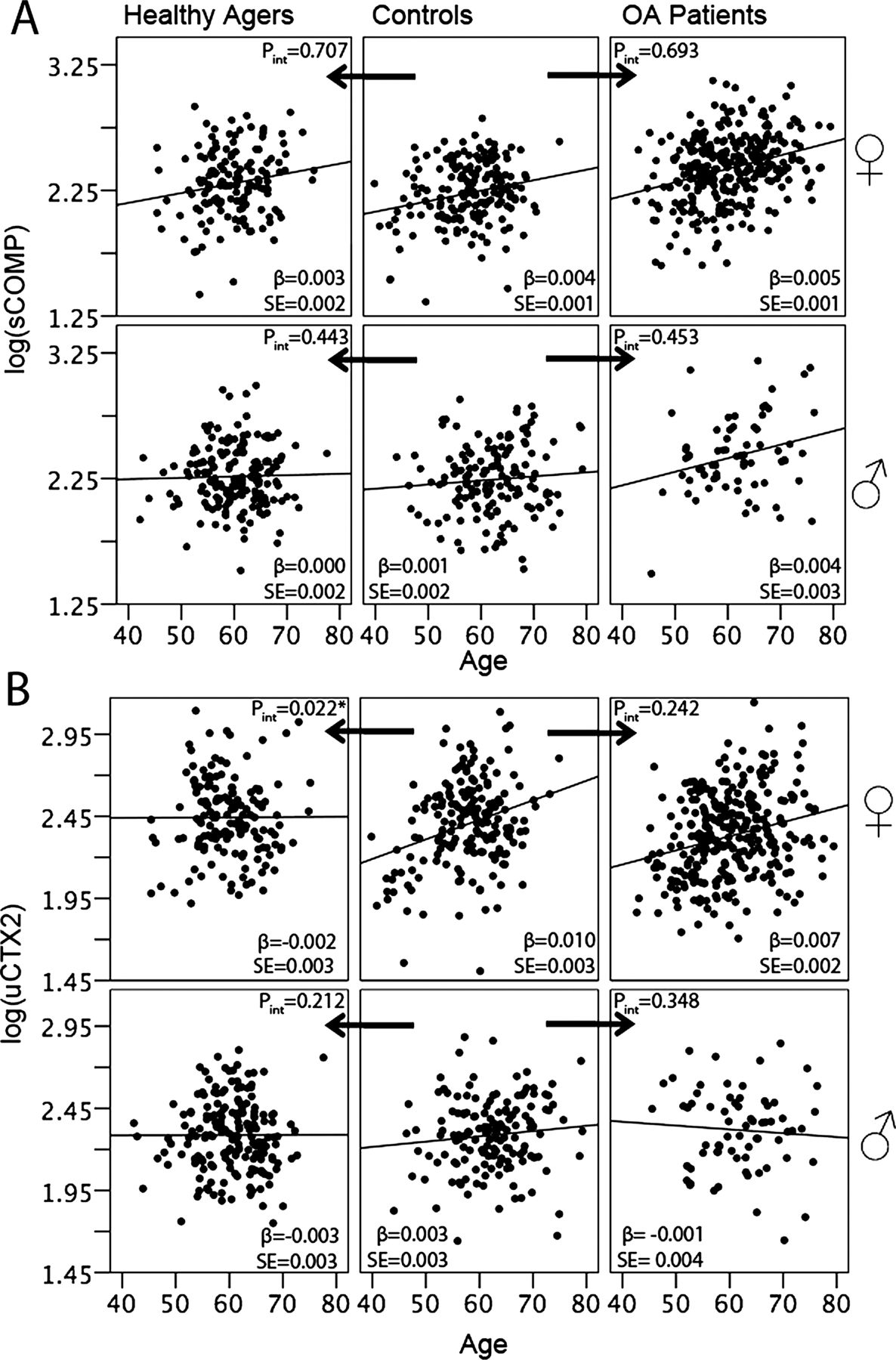
To assess whether the increase in hand ROA with age was also reflected by the potential OA biomarkers, uCTX2 and sCOMP, we plotted these marker levels against age stratified for gender and study group (figure 2A,B). In men, the marker levels did not change significantly with increasing age. In women, sCOMP increased with age independently of hand ROA, which was significant for the controls and patients with OA. The effect size increased from healthy agers (β=0.003, p=0.114) via controls (β=0.004, p=0.006) to GARP patients (β=0.005, p<0.001) (figure 2A). Remarkably, uCTX2 levels in healthy ageing women showed no increase with age (β=−0.002, p=0.616, figure 2B), whereas such an increase was observed in controls and GARP patients independently of hand ROA (β=0.010, p=0.004 and β=0.007, p<0.001, respectively, figure 2B). Quite unexpectedly, the latter rate was similar between the controls and patients with OA. Moreover, the difference between the increase in uCTX2 with age between healthy agers and controls was significant (βinteraction=−0.0113, p=0.022, figure 2B). This indicates that metabolic health, as assessed in healthy agers, independently influences hand ROA characteristics and age-related properties of uCTX2 levels.
{kind=link}
{kind=link}
Scatterplots of serum cartilage oligomeric protein (sCOMP) (A) and urinary cross-linked C-telopeptide of type 2 collagen (uCTX2) (B) level against age, stratified by sex and study group: healthy agers (left), controls (middle) and patients with osteoarthritis (OA) (right). Top panes represent women, bottom panes represent men. Arrows indicate p value of interaction term of age×group testing for differences in increases with age between groups. β, unstandardised β estimate of regression, adjusted for hand radiological osteoarthritis score; SE, standard error of β estimate.
Hand ROA and metabolic health reflected by glucose levels
Finally, in the cross-sectional design, we investigated whether the attenuated age-related increase in hand ROA among female healthy agers compared with controls was influenced by glucose levels as a representative of metabolic health. According to data published previously,11 ,12 indicating that low glucose is a marker of a beneficial metabolic profile, we selected female healthy agers who had a non-fasted glucose level below the mean of all female healthy agers. Online supplementary figure S1 shows a smaller increase in hand ROA with increasing age in female healthy agers with low glucose levels (β=0.032) than in all female healthy agers (β=0.126) and the control group (β=0.201). Only the latter difference is significant (βage×group interaction=−0.186, p=0.013; see online supplementary figure S1). These observations indicate that low glucose is associated with a lower risk of hand ROA in healthy agers. No associations between uCTX2 and glucose metabolism were observed.
Discussion
In this cross-sectional study, we show that middle-aged members of longevity families representing healthy agers, compared with their partners of similar age and BMI, representing controls, have a lower mean number of hand joints with ROA. Furthermore, we show that these healthy agers have a low age-related increase in hand ROA-affected joints and, independently of this, an attenuated age-related increase in uCTX2. These effects were most pronounced in women. Finally we show that healthy ageing women with a low serum glucose level have the lowest age-related increase in hand ROA.
These results indicate that metabolic health in longevity families, as represented by low glucose levels and other previously reported features,11 ,12 may protect against age-related cartilage degeneration and OA. The underlying mechanism may be through lower non-enzymatic glycosylation of the cartilage given the lower availability of glucose. Non-enzymatic glycosylation is known to play a role in ageing cartilage and its decrease in resilience to shear forces.17 ,18 However, further investigation of the healthy ageing phenotype in relation to hand ROA is needed to identify the role of different metabolic components of, for example, lipid metabolism and insulin signalling in the development of hand ROA.
Furthermore, women with a healthy ageing signature appear to have no age-related increase in uCTX2, independently of a smaller increase in hand ROA scores with age. Possibly, the absence of such an increase may mark healthy ageing in the female participants from the LLS, indicating that uCTX2 as a marker of radiographic cartilage breakdown may serve as an independent marker of metabolic health or other aspects of the healthy ageing phenotype. Alternatively, since different studies have indicated that uCTX2 may also reflect changes in bone turnover,9 ,19 the observed changes in uCTX2 characteristics with age in healthy ageing women may also be a reflection of a beneficial bone metabolism. In contrast, we showed that the female patients from the GARP Study exhibit a similar age-related increase in uCTX2 to controls independently of hand ROA, further indicating that the increase in uCTX2 levels does not specifically mark the symptomatic OA phenotype as defined in the GARP Study. We cannot exclude that the remaining age-related uCTX2 increase in the LLS may be attributable to OA at other joint sites, since these were not assessed.
For sCOMP levels, we show that the healthy agers have a significantly higher mean level than the controls; however, this difference was not independent of hand ROA, which correlated significantly and positively with sCOMP levels in the controls, but this correlation was absent in healthy agers. Possibly, the absence of sCOMP association with hand ROA scores in the healthy agers may reflect an intrinsic difference in the metabolic state of the cartilage of healthy agers and controls. The latter hypothesis is highly speculative and acquired from a cross-sectional study design, and hence needs careful consideration in a longitudinal study. Furthermore, for women, we observed a strong age component in the sCOMP levels in all study groups, indicating that age is an important factor to take into account in analyses of this marker in women.
Although men from the LLS did not show significant differences in sCOMP or uCTX2 levels overall or with respect to age, a tendency for sCOMP levels to increase with age is present. Furthermore, a tendency for higher numbers of ROA-affected hand joints at higher age in men was present. It should be noted that, in all study groups, fewer men had hand ROA, in line with the observed prevalence in the general population.
Although the male healthy agers and female controls were slightly older, given the age range analysed, we had enough power to observe differences in levels at increasing ages in both groups. We did not compare the published mean levels of sCOMP and uCTX2 of the GARP Study9 with the mean levels of the LLS, since the biochemical markers were measured in different batches, although the assays in both groups passed the same quality tests for intra- and inter-assay variation and were linear in behaviour. We assessed the number of hand joints with ROA because this is most prevalent and sensitive to changes in the age range of these study groups, thereby allowing analyses of the age-related changes and influences of hand ROA on marker levels. The hand ROA data were assessed between 2 and 4 years after assessment of the biochemical marker level, and, although hand ROA incidence and progression is in general low over such time periods,16 ,20 direct relationships between hand ROA score and marker levels may have been missed in the present analysis. Using a summed score for OA features may be less sensitive for detecting associations between specific OA features and biochemical marker levels.8 Furthermore, we cannot exclude influences of ROA at other joint sites, such as hips or knees, previously reported to influence levels of markers.21 Given the age range, in women, the menopause may influence hand ROA prevalence; however, the relationship is as yet inconclusive and not controlled for in our data.22
In conclusion, this is the first study to report that the age-related increase in prevalence of hand ROA is attenuated in healthy ageing subjects compared with controls of similar age and BMI. In addition, our results show that glucose levels, as a representative of metabolic health, may partly underlie this effect. Furthermore, we show important metabolic and chronological age properties of the potential OA biomarkers, sCOMP and uCTX2, which should be taken into consideration when used in the diagnosis and monitoring of OA. From our study, we conclude that assessment of metabolic health and age are vital when interpreting potential OA biomarkers in the development of effective disease-modifying treatments.
Acknowledgments
We thank all participants of the Leiden Longevity Study and the GARP Study. We acknowledge the TREAT∼OA consortium for financial support. The research leading to these results has received funding from the European Union's Seventh Framework Programme (FP7/2007-2011) under Grant Agreement No 259679, the Dutch Arthritis Association (DAA 2010_017), and was supported by a grant from the Innovation-Oriented Research Programme on Genomics (SenterNovem IGE05007), the Centre for Medical Systems Biology, the Netherlands Consortium for Healthy Ageing (Grant 050-060-810), all in the framework of the Netherlands Genomics Initiative, Netherlands Organization for Scientific Research (NWO).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
- Data supplement 2 - Online methods
- Data supplement 3 - Online table
Footnotes
-
Handling editor Tore K Kvien
-
Contributors SDB, MB, IM, ABM, MK and PES were involved in the conception and execution of this study. W-YK, ACB-J and MAK were involved in data collection. All authors were involved in preparation of the manuscript.
-
Funding Netherlands Consortium for Healthy Ageing.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Medical ethics committee LUMC.
-
Provenance and peer review Not commissioned; externally peer reviewed.