Article Text

Abstract
Objective To establish an easy and practical assay for identifying systemic interferon (IFN) type I bioactivity in patients with primary Sjögren's syndrome (pSS). The IFN type I signature is present in over half of the pSS patients and identifies a subgroup with a higher disease activity. This signature is currently assessed via laborious expression profiles of multiple IFN type I-inducible genes.
Methods In a cohort of 35 pSS patients, myxovirus-resistance protein A (MxA) was assessed as a potential biomarker for type I IFN activity, using an enzyme immunoassay (EIA) on whole-blood and flow cytometric analyses (fluorescence-activated cell sorting, FACS) of isolated CD14 monocytes. In addition, potential biomarkers such as CD64, CD169 and B cell-activating factor (BAFF) were simultaneously analysed in CD14 monocytes using FACS. The IFNscore, a measure for total type I IFN bioactivity, was calculated using expression values of the IFN type I signature genes—IFI44, IFI44L, IFIT3, LY6E and MX1—in CD14 monocytes, determined by real-time quantitative PCR.
Results IFNscores correlated the strongest with monocyte MxA protein (r=0.741, p<0.001) and whole-blood MxA levels (r=0.764, p<0.001), weaker with CD169 (r=0.495, p<0.001) and CD64 (r=0.436, p=0.007), and not at all with BAFF protein. In particular, whole blood MxA levels correlated with EULAR Sjögren's Syndrome Disease Activity Index scores and numerous clinical pSS parameters. Interestingly, patients on hydroxychloroquine showed reduced MxA levels (EIA, p=0.04; FACS p=0.001).
Conclusions The MxA assays were excellent tools to assess IFN type I activity in pSS, MxA-EIA being the most practical. MxA levels associate with features of active disease and are reduced in hydroxychloroquine-treated patients, suggesting the clinical applicability of MxA in stratifying patients according to IFN positivity.
- Sjøgren's Syndrome
- Disease Activity
- Treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Primary Sjögren's syndrome (pSS), the second most common systemic autoimmune disease, is characterised by lymphocytic infiltrates in the salivary and lachrymal glands. Clinical manifestations range among others from ocular and oral dryness to vasculitis and severe fatigue. To date, effective therapy is not available and treatment has been mainly symptomatic. The aetiology of pSS is largely unknown, but evidence for a role of interferon (IFN) type I in the pathogenesis of pSS has been emerging.1–12 Further unravelling the complex pathophysiology of pSS is essential for finding disease-related biomarkers and identifying new treatment targets.
Previously, we described the systemic upregulation of IFN type I-inducible genes (IFIGs) in CD14 monocytes of pSS patients, the so-called IFN type I signature.7 The signature is not restricted to monocytes, as a similar IFN type I signature has been observed in pSS peripheral blood mononuclear cells (PBMCs).12 ,13 Assessment of the IFN type I signature is, however, a laborious real-time PCR technique for the expression of multiple IFIGs and at present, another reliable immunoassay for detection of type I IFNs in blood or serum is not available. The latter is mainly due to the presence of multiple subtypes of IFN type I.5 ,14 ,15 An easy and functional assay to determine the presence of IFN type I activity in the circulation would facilitate the identification of pSS patients with IFN type I signature and further contribute to unravelling the role of IFN type I in pSS patients.
The IFN type I signature, as defined by us, resulted from a factor analysis of multiple tested IFIGs and showed five genes—IFI44L, IFI44, IFIT3, LY6E and MX1—to predict 95% of the total variance of a large set of IFIGs. These five genes were used to calculate an IFN type I expression score (IFNscore) per subject. Recently, we showed this IFN type I signature in pSS monocytes to be associated with higher EULAR Sjögren's Syndrome Disease Activity Index (ESSDAI) scores as well as higher autoantibody production, rheumatoid factor and serum IgG, lower C3 complement levels and higher B cell-activating factor (BAFF) gene expression.13
The IFN type I signature is also displayed by subgroups of patients with systemic sclerosis (SSc), systemic lupus erythematosus (SLE), dermatomyositis and rheumatoid arthritis. Several biomarkers for IFN type I activity have been proposed, among others are MxA, CD64 and CD169.15–24 However, these protein markers have never been tested systematically and simultaneously in a single (pSS) patient group.
MxA (Myxovirus-resistance protein 1) is a key mediator of the IFN-induced antiviral response and is tightly regulated by type I IFNs.25–27 In SSc, MxA gene expression was proposed as a biomarker for type I IFN bioactivity and found to correlate with disease activity.15 Several methods for detection of MxA have been previously described.15 ,19 ,28 ,29 Vallittu et al19 evaluated their enzyme immunoassay (EIA) for MxA in whole blood for monitoring IFN type I bioactivity in multiple sclerosis (MS) patients treated with IFN-β. The MxA-EIA was considered by the authors to be a faster and more reliable method compared with flow cytometric analysis of MxA in PBMCs. To our knowledge, MxA-EIA has never been used for the detection of IFN type I activity in systemic autoimmune diseases.
In this study, we tested MxA as a candidate biomarker for systemic IFN type I activity in pSS using EIA and flow cytometry in whole blood lysates and CD14 monocytes, respectively. In addition, the expression of CD64 (Fcγ RI), CD169 (Siglec-1) and BAFF proteins were simultaneously assessed in CD14 monocytes, as these markers have also been proposed as biomarkers for IFN type I bioactivity in systemic autoimmunity.21–23 ,30
Patients and methods
Patients
According to the 2002 American-European criteria, 35 patients positively diagnosed with pSS were recruited.2 Patients treated with high-dose prednisone (>10 mg daily), immunosuppressants or biologicals were excluded. Level of disease activity was assessed using ESSDAI.31 Twenty-seven healthy controls (HCs), neither suffering from autoimmune diseases nor using corticosteroids, were included. Study subjects were screened to be free of symptoms of underlying viral infections at inclusion (table 1). The medical ethical review board of the Erasmus MC Rotterdam approved the study and written informed consent was obtained.
Patient and control characteristics
Blood collection, preparation and monocyte isolation
Blood samples were collected in clotting tubes for serum preparation (stored at −80°C) and in sodium heparin tubes (Greiner Bio-One, Germany). From heparinised blood, PBMCs and consecutively CD14 peripheral blood monocytes were isolated as previously described.32
Measurement of complements, immunoglobulin levels and autoantibodies
C3 and C4 complements, immunoglobulin levels (such as IgG, IgM and IgA) and anti- Sjögren's syndrome (SS) A/B autoantibody levels were measured as described previously.13
Real-time quantitative PCR
Total RNA was isolated from purified CD14 monocytes using RNeasy columns (Qiagen, Hilden, Germany), subsequently reverse-transcribed to cDNA using a high-capacity cDNA Reverse Transcription Kit and real-time PCR analysis using predesigned primer/probe sets (Applied Biosystems, Foster City, California, USA).32 For calculation of relative expression, all samples were normalised to expression of the household gene Abl. 33Fold change values were determined from normalised CT values (CT gene – CT housekeeping gene) using the Comparative CT (2–ΔΔCT) method (User Bulletin #2, Applied Biosystems, Foster City, California).
Flow cytometry
Fluorescence-activated cell sorting (FACS) analysis was used to determine surface expression and intracellular cytokine content in purified CD14 monocytes. Membrane staining was performed with fluorescently labelled antibodies: anti-CD14 (APC/Cy7; BD Biosciences, California, USA), and either anti-CD64 (PE; Serotech, Toronto, Canada) or CD169 (Alexa Fluor-647; Serotech) were incubated in the dark for 20 min. Subsequently, cells were fixed (1% paraformaldehyde), permeabilised (0.5% saponin) and stained with either anti-BAFF (FITC; R&D Systems, Philadelphia, Pennsylvania, USA) or unconjugated anti-MxA (ProteinTech Group, Chicago, Illinois, USA), incubated in the dark for 30 min on ice; secondary antibody was goat-anti rabbit-FITC (Supertech). Unstained cells and appropriate isotype-matched controls (BD Biosciences) were used to confirm antibody specificity. Fluorescence was assayed using four-colour flow cytometry (FACS CaliburBeckton Dickinson & co, San Jose, California, USA) and analysed using FlowJo Software (TreeStar Inc, USA).
MxA EIA
MxA-EIA was executed as previously described.19 Heparinised blood (25 μl) was lysed 1:20 and stored at −70°C until assayed.19 Briefly (see online supplementary figure S1 for full description), lysed whole blood samples and biotinylated detector-monoclonal antibody (MAb) were loaded onto MAb-coated micortitre strips and incubated overnight at 8°C; colour reaction was stopped, absorbance450 was measured and [MxA] read from a master standard curve. Detection limit was 10 μg/l and determined as three times the SD of eight negative control replicates.26
IFNscore
Monocyte IFN type I signature was defined by the relative expression of five IFIGs: IFI44L, IFI44, IFIT3, LY6E and MxA.13 MeanHC and SDHC of each gene in the HC group were used to standardise the expression levels. IFNscores per subject represent the sum of these standardised scores, calculated as previously described.34 ,35 IFNscore distribution for the 35 patients was bimodal, with an overlap at a score of 10. Furthermore, HC only occasionally showed an IFNscore≥10; consequently, values of 10 or more represent IFN type I signature positivity.13
Statistical analysis
Comparisons were analysed using the non-parametric Mann–Whitney U test to compare medians, and an independent t test was used to compare the means (for normally distributed data). For correlation studies, the Spearman's rho (rs) or Pearson's correlation coefficient (rp) were calculated. Values of p<0.05 were considered statistically significant. For multiple variable testing, values of p<0.01 (p<0.05/5) were considered statistically significant after applying a Bonferroni correction (n=5). Multiple group comparisons were analysed using the Kruskal–Wallis test; statistical analysis was performed using SPSS V.17.0.
Results
Stratification of pSS patients into IFN type I signature positive and negative patients
We used our previously described definition for the IFN type I signature13 and reconfirmed the presence of the signature in the current cohort—using the five indicator genes IFI44L, IFI44, IFIT3, LY6E and MX1 (figure 1A). We stratified the patient group as previously described in patients positive for the IFN type I signature (IFNpos; IFNscore≥10) and patients negative for the signature (IFNneg; IFNscore<10). Using this paradigm, none of the HC scored above 10, whereas 21 out of 35 pSS patients were IFNpos—a prevalence of 60% (figure 1B). In figure 1C, gene expression for the five signature genes is depicted in a heat map.

(A) Relative mRNA gene expression is shown for the five IFN type I inducible genes of the IFN type I signature in CD14 monocytes of primary Sjögren's syndrome (pSS) patients (n=35) and healthy controls (HCs) (n=27). Patient group is stratified in patients negative for the IFN type I signature (signature negative, IFNneg) (n=14) and patients positive for signature (IFN type I signature positive, IFNpos) (n=21). (B) The IFNscore is shown for HC and pSS patients. A cut-off value of 10 is used as threshold for IFNneg (IFNscore<10) and IFNpos (IFNscore≥10) pSS patients. Each symbol represents an individual sample; horizontal lines represent the median. p Values are shown, and to compare medians the Mann–Whitney U test was used. (C) Heat map depicting gene expression of IFN type I-inducible genes. Individual study subjects sorted according to increasing IFNscore (scale from blue to red) and stratified in HC (left), IFNneg (right upper panel) and IFNpos pSS patients (lower panel).
MxA correlates strongly to IFN type I bioactivity in pSS
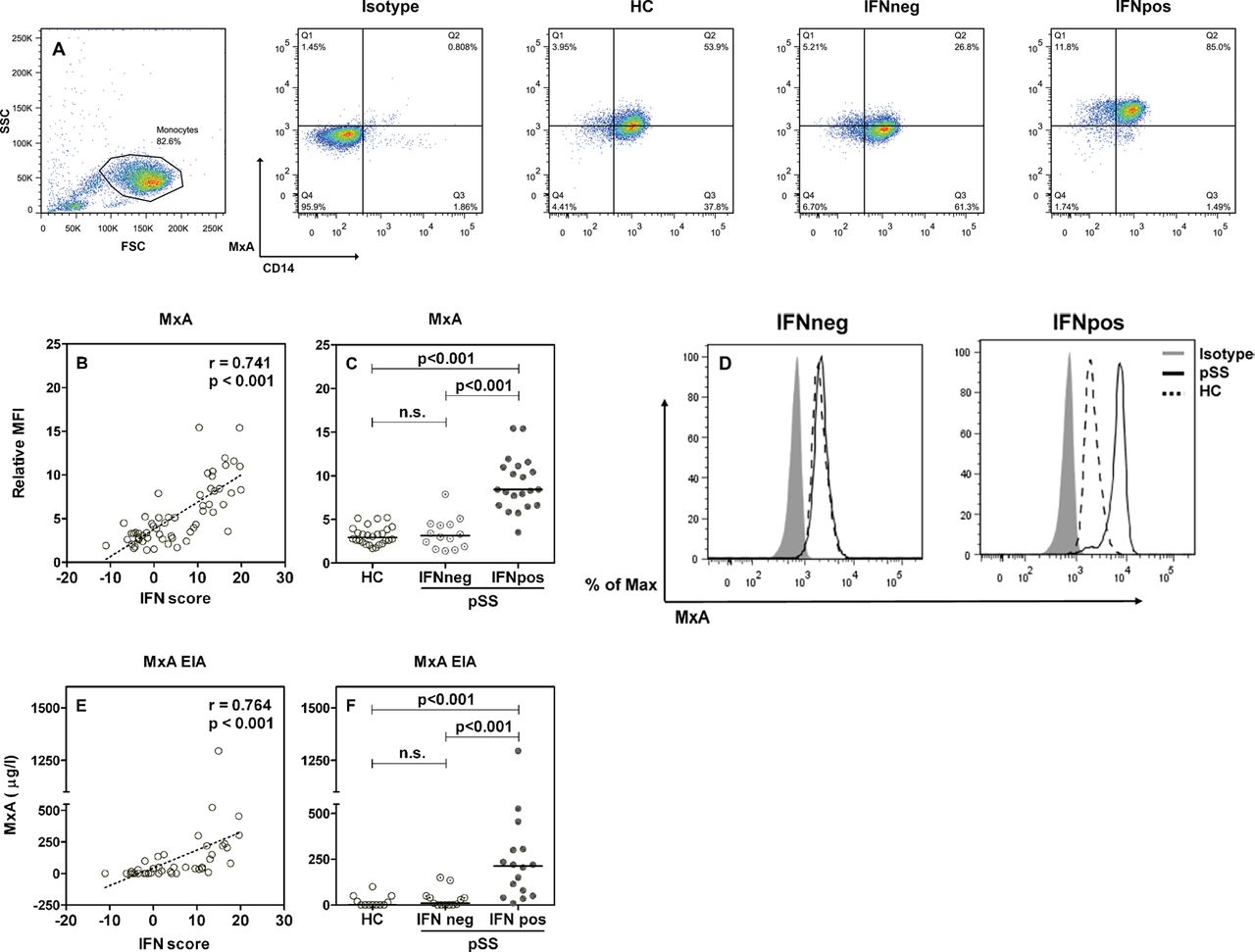
To assess MxA protein as a potential biomarker for the IFN type I signature, intracellular MxA was measured in CD14 monocytes using flow cytometry and in whole-blood lysates using MxA-EIA.
Significant positive correlation was observed between the IFNscores and intracellular MxA levels, as assessed by flow cytometry (figure 2B). Relative mean fluorescence intensity scores of MxA were next compared between HC, IFNneg and IFNpos pSS patients. Quantification of CD14 monocyte MxA levels showed a significant increase in IFNpos patients compared with IFNneg patients and HC, whereas IFNneg patients showed MxA levels indistinguishable from HC (figure 2C,D).

Flow cytometric analysis of MxA protein expression in CD14 monocytes from healthy controls (HCs) (n=27) and primary Sjögren's syndrome (pSS) patients stratified in interferon (IFN) type I signature negative (IFNneg) (n=14) and IFN type I signature positive (IFNpos) (n=21) patients. (A) Representative dot plots show CD14 and MxA protein expression on monocytes from study subjects. (B) Correlation plot shown between IFNscores for all study subjects and relative mean fluorescent intensity (MFI) of MxA. (C) Relative MFI of MxA is shown for healthy controls (HCs), IFNneg and IFNpos pSS patients. (D) MxA levels are shown for IFNneg (left) and IFNpos (right) pSS patients. Representative histograms are depicted; shaded histogram represents the isotype control, dotted line represents the HC and the solid line represents the pSS patients. Relative expression was calculated as MxA-specific staining (MFI)/isotype control (MFI). MxA levels (µg/l) determined by MxA-enzyme immunoassay (EIA) in whole-blood lysates of HC and pSS patients. (E) Correlation plot between IFNscores for all study subjects and intracellular MxA-EIA (µg/l) levels. (F) MxA-EIA (µg/l) levels shown for HC and pSS patients, stratified in IFNneg and IFNpos patients. Each symbol represents an individual sample (duplicates of two separate EIA measurements per study subject); horizontal lines represent the median. The correlation coefficients (r) and p values are shown. For correlations, Spearman's rho correlation test was used and to compare medians, the Mann–Whitney U test was used.
Using the MxA-EIA, MxA protein levels (μg/l) were assessed in lysed whole blood of the same study subjects. Correlating whole blood MxA levels to IFNscores showed a significant positive correlation (figure 2E). IFNpos patients showed significantly elevated MxA protein levels, compared with IFNneg patients and HC. An increase was not observed in IFNneg patients, again showing MxA levels equal to HC (figure 2F).
CD64 and CD169 correlate weakly to IFN type I bioactivity in pSS
We also assessed surface protein levels of CD64 and CD169 (other proposed biomarkers of IFN activity) on CD14 monocytes using flow cytometry (see online supplementary figure S2). A significant positive correlation was observed between the IFNscore and surface expression of CD64 (figure 3A) and CD169 (figure 3B), respectively, though with considerably lower correlation coefficients as found for MxA (figure 2).
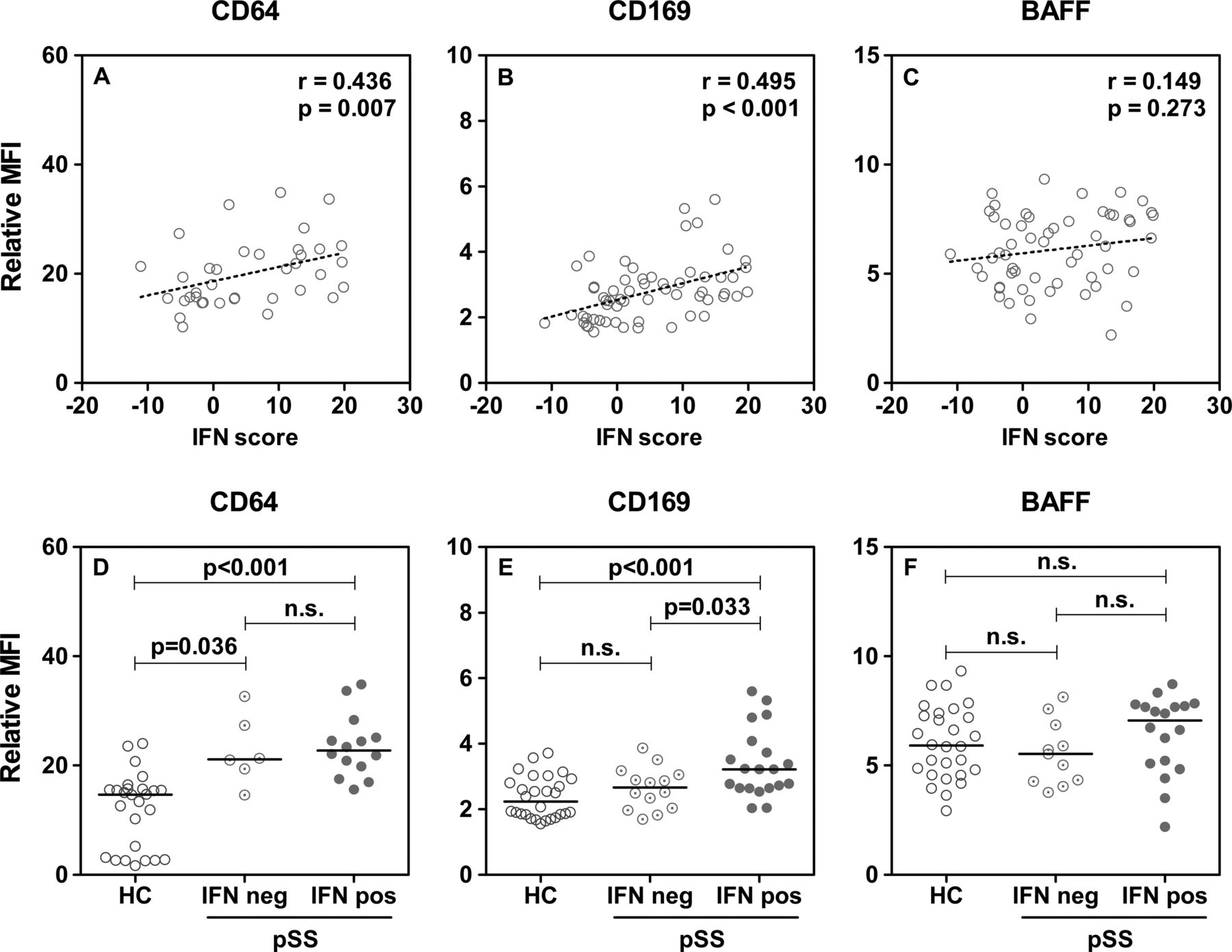
Flow cytometric analysis of CD14 monocytes from healthy controls (HCs) and primary Sjögren's syndrome (pSS) patients. Correlation plots shown between interferon (IFN) scores for all study subjects and (A) CD64, (B) CD169 and (C) B cell-activating factor (BAFF) protein levels, respectively. Relative mean fluorescent intensity (MFI) for (D) CD64 (E) CD169 and (F) BAFF protein levels are shown for CD14 monocytes from HC (n=27) and pSS patients, stratified in IFN type I signature negative (IFNneg) (n=14) and IFN type Isignature positive (IFNpos) (n=21) patients. Each symbol represents an individual sample; horizontal lines represent the median. Relative expression was calculated as protein-specific staining (MFI)/isotype control (MFI). The correlation coefficients (r) and p values are shown. For correlations on CD64 and CD169, Spearman's rho correlation test was used and to compare medians, the Mann–Whitney U test was used. For BAFF, Pearson's correlation test was used and to compare means, the independent t test was used.
Figure 3D shows CD64 upregulation on monocytes of pSS patients irrespective of their IFN positivity. For CD169 surface expression, this was not the case as the marker was solely upregulated in IFNpos pSS patients (figure 3E).
BAFF protein does not correlate to IFN type I bioactivity in pSS
Previously, we established a positive correlation for the presence of the IFN type I signature and BAFF mRNA gene expression in CD14 monocytes.13 This observation was confirmed in our current cohort (see online supplementary figure S3). We therefore assessed intracellular BAFF protein in CD14 monocytes as a candidate biomarker for IFN type I, using flow cytometry. Intracellular BAFF levels showed no correlation with the IFNscore (figure 3C; see online supplementary figure S2). Moreover, BAFF protein levels were not significantly elevated in pSS patients compared with HC, neither in IFNpos nor IFNneg patients (figure 3F).
MxA correlates with disease manifestations of pSS
Previously observed association of the IFN type I signature with high ESSDAI disease activity scores13 (reconfirmed in this study; figure 4A) gave rise to the question whether this also holds true for the here described potential biomarkers MxA, CD64 and CD169. We were able to assess ESSDAI disease activity scores in 23 pSS patients of this cohort. Significant correlation was observed between ESSDAI scores and MxA levels measured by either assays, even though the correlation was the strongest when the EIA was used (table 2 and figure 4B,C). For the other biomarkers, no correlation was found (see online supplementary table S1).
Comparisons of the MxA biomarker—assessed by MxA-EIA and MxA-FACS—with clinical and laboratory parameters of pSS patients

{kind=link}
{kind=link}
{kind=link}
{kind=link}
EULAR Sjögren's Syndrome Disease Activity Index (ESSDAI) scores stratified in (A) interferon (IFN) type I signature negative (IFNneg) and IFN type I signature positive (IFNpos) primary Sjögren's syndrome (pSS) patients (B) MxA (μg/l) levels as measured by the MxA-EIA; MxA<100 μg/l (low) and MxA>100 μg /l (high). Cutoff values were determined as meanHC + 2×SDHC (C) Correlation plot is shown between EULAR Sjögren's Syndrome Disease Activity Index (ESSDAI) scores and MxA (μg/l) levels. (D) MxA (μg/l) levels in pSS patients in presence (+) or absence (−) of autoantibodies; anti-SSA (divided in Ro52 and Ro60) and anti-SSB (E) immunoglobulin levels (g/l) such as IgG, IgA and IgM in pSS patients stratified in MxA<100 μg /l and MxA>100 μg/l. Comparisons for pSS patients in presence (+) or absence (−) of hydroxychloroquine (Plaquenil) treatment plotted for (F) the IFNscore; line represents IFNscore cutoff ≥10, (G) MxA (μg/l), as measured by the MxA-EIA and (H) ESSDAI scores. Each symbol represents an individual sample; horizontal lines represent the median. The correlation coefficient (r) and p values (*p>0.05; **p>0.01; ***p>0.001) are shown, Spearman's rho correlation test was used and to compare medians, the Mann–Whitney U test was used.
We subsequently determined whether the potential biomarkers were associated with classical aberrant immune parameters of pSS such as anti-SSA and anti-SSB autoantibodies, rheumatoid factor, immunoglobulin levels and neutrophil counts (table 2). In particular, whole blood MxA levels showed the strongest and the most significant correlations with many of these parameters; patients with autoantibodies showed higher levels of whole blood MxA compared with patients free of autoantibodies (figure 4D). Significant positive correlations were also found between whole-blood MxA and rheumatoid factor, and immunoglobulin levels (IgG, IgA and IgM) (table 2, figure 4E). Significant negative correlations were found between whole-blood MxA, haemoglobin levels and neutrophil counts. Monocyte MxA(-Facs) and CD169 levels performed less well in these comparisons (table 2; see online supplementary table S1).
Patients on hydroxychloroquine (HCQ, Plaquenil) treatment had significantly reduced biomarkers of IFN activity (figure 4F,G); table 2 and figure 4G show patients on HCQ treatment to have reduced levels of MxA, measured by EIA and FACS. HCQ was, however, found to have no significant effect on ESSDAI levels (figure 4H).
Discussion
Our study is the first to simultaneously assess protein levels of MxA, CD64, CD169 and BAFF as biomarkers for IFN type I detection. Herein, MxA was distinguished as the best functional biomarker for systemic IFN type I activity in pSS.
MxA protein is considered as an important mediator of early innate immune defence and its expression has been used as a marker for IFN bioactivity in experimental as well as clinical settings.19 ,27 The MxA gene, in contrast to other IFIGs, is not directly induced by viruses and strictly depends on IFN signalling.27 Furthermore, the stability of MxA protein in cells was observed to be higher than the corresponding mRNA levels.26 We assessed intracellular MxA protein using an EIA method on whole blood and flow cytometric analyses on circulating CD14 monocytes. In our patients, flow cytometric detection of MxA in monocytes showed a slightly better distinction between IFNpos and IFNneg patients within this pSS group, relative to the EIA in whole blood. Nevertheless, the MxA-EIA was a more practical assay as it requires only 25 µl of whole blood—obtained during routine blood collection and easily stored at −70°C to the time of assessment—without necessity of laborious PBMC isolation and subsequent monocyte isolation. Vallittu et al,19 who previously validated the MxA-EIA for monitoring MS patients treated with IFN-β, concluded the EIA favourable for large-scale clinical application due to its high level of standardisation and reproducibility. We also experienced the EIA to be less variable than FACS (data not shown). This report shows whole-blood MxA levels measured by EIA to have the strongest correlation with features of active pSS, that is, with higher ESSDAI scores, anti-SSA/SSB antibodies, rheumatoid factor, immunoglobulin levels, lower haemoglobulin levels and neutrophil counts. We found no association with complement consumption as previously found for the IFNscore.13 On the basis of these observations, we propose to use the MxA-EIA for identification of IFN type I bioactivity in pSS.
Alongside MxA, we also considered CD64, CD169 and BAFF as candidates, observing a significant correlation between CD64 and CD169 and the IFNscore, be it with a relatively low correlation coefficient.
CD64, the high-affinity Fc-gamma receptor I (Fcγ RI) recognising Fc portion of IgG, is exclusively expressed on myeloid cells and found to correlate with IFIG expression in SLE.21 ,23 Levels of CD64 on monocytes did neither correlate with IFN type I activity, nor with the clinical and laboratory parameters. In contrast, the surface marker was overexpressed in all pSS patients. We therefore consider it as a marker of systemic autoimmunity in general.36
CD169, also termed sialoadhesin (Siglec-1), previously identified as a biomarker for IFN type I activation in SLE, was found to correlate with disease severity.16 Also in SSc, elevated CD169 levels were found on monocytes.17 In our hands, CD169 was elevated in IFNpos pSS patients and correlated to several clinical and laboratory parameters, even though not as strongly as the MxA assays.
BAFF overexpression has been observed in serum, salivary glands and monocytes in pSS patients.18 ,20 ,37 ,38 We previously observed a strong correlation between the IFN type I signature and BAFF mRNA in pSS monocytes.13 Moreover, we found BAFF serum protein level increased in pSS compared with HC, but did not find a correlation with the IFNscore; additionally, BAFF serum protein did not correlate with BAFF mRNA. We report here that BAFF protein levels showed a slight but not significant increase in IFNpos patients, whereas BAFF mRNA was indeed significantly increased in IFNpos patients. This again indicates the lack of correlation between BAFF mRNA and BAFF protein.
Some limitations of our study are for one, the relatively small sample size for CD64. Assessing this surface marker in a large set of patients is warranted to better understand its role in systemic autoimmunity. Second, MxA-EIA levels were not assessed for all subjects due to whole-blood necessity. Furthermore, absence of viral infections was defined as ‘no symptoms of underlying viral infections’ at inclusion, whereas no viral screening was done to confirm. In HC with relatively high MxA levels, however, ENA profiles were run to rule out the presence of autoantibody. Third, the ESSDAI as well as some clinical and laboratory parameters were not assessed in all pSS patients.
In this study, we reconfirmed a monocyte IFN type I signature prevalence in over half of the pSS patients, a subgroup with higher disease activity.13 We proposed the identification of these subgroups useful in establishing a patient's eligibility for specific treatments. Indeed, an interesting finding here was that patients on HCQ treatment had considerably reduced MxA levels, indicating HCQ to perhaps interfere with IFN production. A recent report shows HCQ to impair systemic IFNα production.39 Our data suggest that identifying the IFN type I signature by performing MxA assays might prove useful in predicting HQC treatment responsiveness. In this cohort, there are more HCQ users in the IFNneg group compared with IFNpos. However, it is not likely that the increased ESSDAI levels in the IFNpos group are an effect of less HCQ use in this group, because in the IFNpos group, 62% of the patients use HCQ and are nevertheless IFNpos. Moreover, we previously showed 61% (23/38) of the IFNpos patients to use HCQ compared with 55% (17/31) of IFNneg patients. In addition, HCQ use did not significantly affect ESSDAI scores (figure 4H). Larger studies are, however, warranted to fully elucidate the effects of HCQ on the IFN type I system, in particular, longitudinal studies monitoring MxA levels in HCQ-naïve patients starting HCQ treatment.
The association between the IFN type I signature, MxA protein and disease activity levels in pSS needs to be further assessed, by for one looking longitudinally, in order to validate MxA as a disease activity marker. The same holds true for association between IFN type I polymorphisms and MxA, as these polymorphisms have been linked to increased IFNα sensitivity.40 ,41
To determine the applicability of the MxA-EIA in other IFN type I-related diseases, MxA levels were assessed in a small SLE cohort (see online supplemental figure S4) and showed results similar to pSS—a significant correlation between IFNscores and MxA levels (r=0.885, p<0.0001)—suggesting a broad applicability of MxA-EIA in systemic autoimmunity.
In conclusion, we identify MxA protein expression by EIA and FACS analysis as practical and rapid approaches for assessment of IFN type I bioactivity in pSS. MxA-EIA is the simplest and most reliable of these assays and indicates clinical applicability in stratifying pSS patients according to IFN positivity. The use of MxA as a biomarker for identifying patients eligible for therapy in pSS clearly requires further research.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figures
Footnotes
Handling editor Tore K Kvien
NIM and ZB share first authorship.
-
Acknowledgements The authors acknowledge Ms M Kivivirta (University of Turku, Finland) for her technical assistance in running the MxA-EIAs, Dr M Schreurs (Erasmus MC Rotterdam, The Netherlands) for measurement of complement, immunoglobulin levels and autoantibodies and Msc. W Beumer (Erasmus MC Rotterdam, The Netherlands) for his scientific perspective as well as aid in figure design.
-
Contributors NIM and ZB (guarantors) were involved in conception and study design, overall data acquisition and monitoring, analysis and interpretation of data, drafting and revising the article. MW was involved in laboratory data acquisition, analysis and interpretation and revising the article. CGvH-M and KH were involved in laboratory data acquisition and analysis, and revising the article. JPvdM, PLvD and VASHD were involved in clinical data acquisition and interpretation, and revising the article. HAD was involved in conception and study design, interpretation of data and revising the article. MAV (guarantor) was involved in conception and study design, data monitoring and interpretation and revising the article. All authors approved the final version.
-
Funding This study was supported by grants from the Dutch Arthritis Foundation (Reumafonds);10-1-401 and the Netherlands Organisation for Scientific Research (NWO; 017.007.095).
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The Medical Ethical Review Board of the Erasmus MC Rotterdam.
-
Provenance and peer review Not commissioned; externally peer reviewed.