Article Text

Abstract
Objectives To compare the effects of an intermediate molecular weight (MW) intra-articular hyaluronic acid (HA) with a low MW product on knee osteoarthritis (OA) symptoms.
Methods Patients with symptomatic knee OA were enrolled inarandomised, controlled, double-blind, parallel-group, non-inferiority trial with the possibility to shift to superiority. Patients were randomised to GO-ON(MW 800–1500 kD, 25 mg/2.5 ml) or Hyalgan(MW 500–730 kD, 20 mg/2 ml) injected at 3-weekly intervals. The primary outcome was 6-month change in the WOMAC pain subscale (0–100 mm). Sample size was calculated on a non-inferiority margin of 9 mm, lower than the minimum perceptible clinical improvement. Secondary endpoints included OARSI-OMERACT responder rates
Results The intention-to-treat (ITT) and per-protocol (PP) populations consisted of 217 and 209 patients and 171 and 172 patients in the GO-ON and Hyalgan groups, respectively. ITT WOMAC pain of 47.5±1.0(SE) and 48.8±1.0 mm decreased by 22.9±1.4 mm with GO-ON and 18.4±1.5 mm with Hyalgan after 6 months. The primary analysis was conducted in the PP population followed by the ITT population.Mean (95% CI) differences in WOMAC pain change were 5.2 (0.9 to 9.6)mm and 4.5 (0.5 to 8.5)mm, respectively,favouring GO-ON, satisfying the claim for non-inferiority (lower limit>−9 mm) and for statistical superiority (95% CI all>0, p=0.021). Ahigher proportion of OARSI/OMERACT responders was observed with GO-ONthan with Hyalgan (73.3% vs58.4%, p=0.001). Both preparations were well tolerated.
Conclusions Treatment with 3-weekly injections of intermediate MW HA may be superior to low MW HA on knee OA symptoms over 6 months, with similar safety.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Hyaluronic acid (HA) is a glycosaminoglycan constituent of synovial fluid and cartilage matrix in normal joints. In osteoarthritis, HA molecular weight (MW) and concentration are decreased. Exogenous HA is available as a viscosupplementation device or a drug for intra-articular use in the treatment of knee osteoarthritis symptoms.1 Different HA formulations are currently available worldwide: from the reference low MW preparation (range 500 000–730 000 Daltons) to more recent intermediate MW (range 800 000–2 000 000) and even cross-linked, high MW formulations (average 6 000 000 Daltons) including hylans, non-animal-derived HA and others. However, the efficacy of HA in knee osteoarthritis is still debated, which is reflected in several meta-analyses;2,–,7 the majority suggest small to strong effects of HA,2,–,5 while a minority failed to show a greater effect than placebo.6 ,7 Despite controversies, HA injections are recommended by the current Osteoarthritis Research Society International (OARSI) guidelines and previous practice guidelines.8
While a more recent re-appraisal suggests that there is poor evidence of significant pain relief when the analysis is restricted to high-quality studies,9 one early meta-analysis4 suggested that the large heterogeneity between trials might be caused by the possible greater efficacy of high MW HA products. This was recently negated by a meta-analysis10 in which high MW, cross-linked HA was not significantly superior to lower MW preparations, but had a doubling frequency of post-injection joint flares. In addition, HA was found to have longer-lasting pain control compared with intra-articular corticosteroids, and the majority of trials has been performed with the low MW HA product.11
Low MW HA thus often remains the preferred option when using HA in knee osteoarthritis. However, there is a paucity of appropriately sized, high-quality trials comparing the effects of different MW preparations, with particular regard to potential differences between low and intermediate MW products, given the worse safety profile of high MW formulations.10 The present study was therefore designed to compare the effects of the reference low MW HA product (Hyalgan) with a well-characterised intermediate MW preparation (GO-ON) on knee osteoarthritis symptoms.
Methods
Study design
This was a multicentre (50 orthopaedics and/or rheumatology practice sites in France and Germany), prospective, randomised, double-blind, controlled, parallel-group trial, to compare the efficacy and safety of GO-ON with that of Hyalgan according to a non-inferiority design, with the possibility to shift to superiority following current regulatory guidelines.12 ,13 The trial was registered on the European Medicines Agency database accessible at www.clinicaltrialsregister.eu (EudraCt no 2008-003875-35). Ethics approval was provided by the ethics review boards of the coordinating investigators (co-authors FB and JG) in France and Germany (Comité de Protection des Personnes, AP-HP St-Antoine Hospital, Paris and the ethics committee of Regensburg University, respectively) and by all applicable local ethics committees. After signing an informed consent, patients were screened at least 7 days before randomisation. Patients received 3-weekly injections of the test or comparator preparations (1:1 allocation ratio) and were then seen at weeks 6, 14, 20 and 26, ie, 4, 12, 18 and 24 weeks following the end of treatment.
Patient selection
Patients of either sex, aged 50–80 years, fulfilling the American College of Rheumatology clinical and radiological criteria for knee osteoarthritis,14 were enrolled if they had a history of symptoms for at least 6 months and insufficient/failed response to analgesics and/or regular non-steroidal anti-inflammatory drugs (NSAID), or were intolerant to regular NSAID or weak opioids. Current symptoms (after ≥2 days wash-out from NSAID, including topical agents, or 1 day from non-narcotic analgesics) had to include global knee pain of 40 mm or greater on a 100 mm visual analogue scale (VAS), Western Ontario and McMaster Universities (WOMAC) pain subscale score of 25 or greater on the 0–100 normalised scale and Lequesne index of 4 or greater. x-Rays (past 12 months) had to show Kellgren and Lawrence stage II or III; radiological evidence of bilateral knee osteoarthritis was accepted if global pain VAS in the contralateral knee was less than 30 mm. Main exclusions were: isolated/predominantly patellofemoral symptomatic osteoarthritis, secondary knee osteoarthritis, symptomatic hip osteoarthritis homolateral to the target knee, inflammatory or other rheumatic diseases, clinical joint effusion, excessive (≥8°) varus or valgus knee deformity (at physical examination, as confirmed by standard radiograph).
Treatments, randomisation, allocation concealment and blinding
GO-ON (Rottapharm|Madaus, Monza, Italy) is a preparation of sodium hyaluronate obtained by fermentation from Streptococcus equi, with an intermediate MW (range 800 000–1 500 000 Daltons), presented in 2.5 ml prefilled syringes and a concentration of 10 mg/ml. Hyalgan (Fidia Abano Terme, Italy) is sodium hyaluronate derived from rooster combs, with a low MW (range 500 000–730 000) and a concentration of 10 mg/ml in 2 ml. Both preparations are recommended for cycles of 3–5-weekly injections, but studies have shown no apparent difference between the two regimens with Hyalgan.3 Treatments were therefore administered intra-articularly, using a lateral femoropatellar approach, at 3-weekly intervals.
A block randomisation list was computer-generated and electronically associated to a pack list (each pack containing one syringe) by independent groups who maintained their secrecy, having no contacts with the investigators or personnel involved in the conduct of the study. Blocks were balanced at each site and their size was secret to maintain blinding. Randomisation was centralised by an interactive voice response system: the randomisation call assigned the first available position in the randomisation list and therefore the first treatment pack (identified by a unique number) available at the site. Two additional calls were made to obtain the pack number for the second and third injections. Consequently, there was no possibility for the investigator to predict the next treatment assignment, thus ensuring adequate allocation concealment.
Given the impossibility of obtaining identical presentations of the compared medications, double-blind conditions were obtained by appointing at each site one ‘injector investigator’ in charge of independently administering the treatments and one ‘assessor investigator’ performing all assessments blinded to the treatment. Patient blinding was ensured by avoiding visual access to the injection field (eg, by a screen between the patient and his/her knee). Double-blind conditions were successfully achieved for all patients (as noted in the case record form).
Use of paracetamol up to 4 g per day for four consecutive days was allowed as rescue medication if unbearable pain had not improved after at least 1 h rest. In case of paracetamol failure or contraindication, NSAID could be prescribed for a limited and specified period. Paracetamol or NSAID had to be stopped 24 h or 2 days, respectively, before each assessment visit. Daily consumption of the rescue medication was recorded in a patient diary. No other use of paracetamol or NSAID (excluding aspirin <325 mg/day as antiaggregant) was allowed during the study, similar to opioids, intra-articular or systemic corticosteroids (washout ≥1 and 3 months, respectively), or other HA preparations (washout ≥12 months). Glucosamine sulphate, other glucosamines or other slow-acting drugs for osteoarthritis (eg, chondroitin sulphate, diacerhein or avocado/soybean unsaponifiables) were allowed if at a stable dosage for 3 months or more.
Efficacy outcomes
The pain subscale of the WOMAC osteoarthritis index (VAS version VA3.1) was the study primary endpoint.15 Results were normalised on a 0–100 scale for each domain, with the total index, physical function and stiffness subscales being assessed as secondary endpoints.
Other secondary efficacy endpoints included: global knee pain during the past 48 h on a 0–100 mm VAS; the Lequesne algofunctional index;16 the intermittent and constant osteoarthritis pain (ICOAP) index on the 0–100 score transformation recommended by the OARSI and outcome measures in rheumatology (OMERACT);17 patient global assessment (PGA) on a 100 mm VAS (see supplementary material 2, available online only, for the exact wording of this and the global knee pain VAS question); the proportion of OARSI/OMERACT responders.18 The proportion of patients achieving the minimum clinically important improvement (MCII) and patient acceptable symptom state (PASS)19 ,20 was also calculated for global pain VAS, WOMAC function subscale and PGA. Consumption of the rescue medication was another efficacy endpoint.
Safety assessment
The safety population comprised all patients receiving at least one injection of the study medication. Adverse events (AE) observed by the investigators or reported by the patients spontaneously or following a non-leading question, were coded using the Medical Dictionary for Regulatory Activities. Particular attention was paid to local painful reactions at the injection site, postinjection reactions (eg, effusions) and acute pseudoseptic arthritis.21
Statistical analysis
The primary outcome was the difference in the mean change from baseline on the WOMAC pain subscale score at week 26 (6 months after the end of treatment). The acceptable margin for non-inferiority was preset at −9 mm, ie, less than the minimum perceptible clinical improvement of −10 mm.22 GO-ON would be declared non-inferior to Hyalgan if the lower limit of the 95% CI lies above −9 mm in both the per-protocol (PP) and intention-to-treat (ITT) populations.12 ,13 If the 95% CI also lies above zero in ITT, there is evidence of superiority at the 5% significance level and a two-way analysis of variance (ANOVA) with treatment and study centre as factors provided the actual p value, with no multiplicity argument affecting this interpretation.12 ,13 The effect size was calculated according to Hedges.23
The sample size on this non-inferiority margin was calculated assuming a SD of 23 mm, based on a previous study with Hyalgan24 and conservatively increased by 15%, resulting in 144 patients per group in the PP population to achieve a power of 90% at a significance level of 5%. Assuming a 30% discontinuation rate, this was increased to 200 patients per group in the ITT population, which consisted of all randomly assigned patients with at least one injection and one post-injection assessment of the primary endpoint.25 For drop-outs and other exclusions from the PP population, missing values were replaced by the baseline value, according to the baseline observation carried-forward approach.26
All secondary endpoints were analysed for superiority, as predetermined in the protocol. The changes in the WOMAC total index and its subscales, global knee pain, Lequesne index, PGA, ICOAP index and daily mean rescue medication consumption were analysed by ANOVA as the primary endpoint. The proportions of OARSI/OMERACT responders and patients with MCII or PASS were compared by the χ2 test, similar to the number of patients with AE and those using the rescue medication (worst case approach for drop-outs in the latter case). An analysis at week 14 (12 weeks after the end of treatment), was also performed as exploratory on all parameters. Demographic and baseline characteristics were compared by two-way ANOVA for continuous variables or the Cochran–Mantel–Haenszel test, controlling for study centre, for categorical parameters. Statistical analyses were performed using the SPSS statistical package (version 9.2).
Results
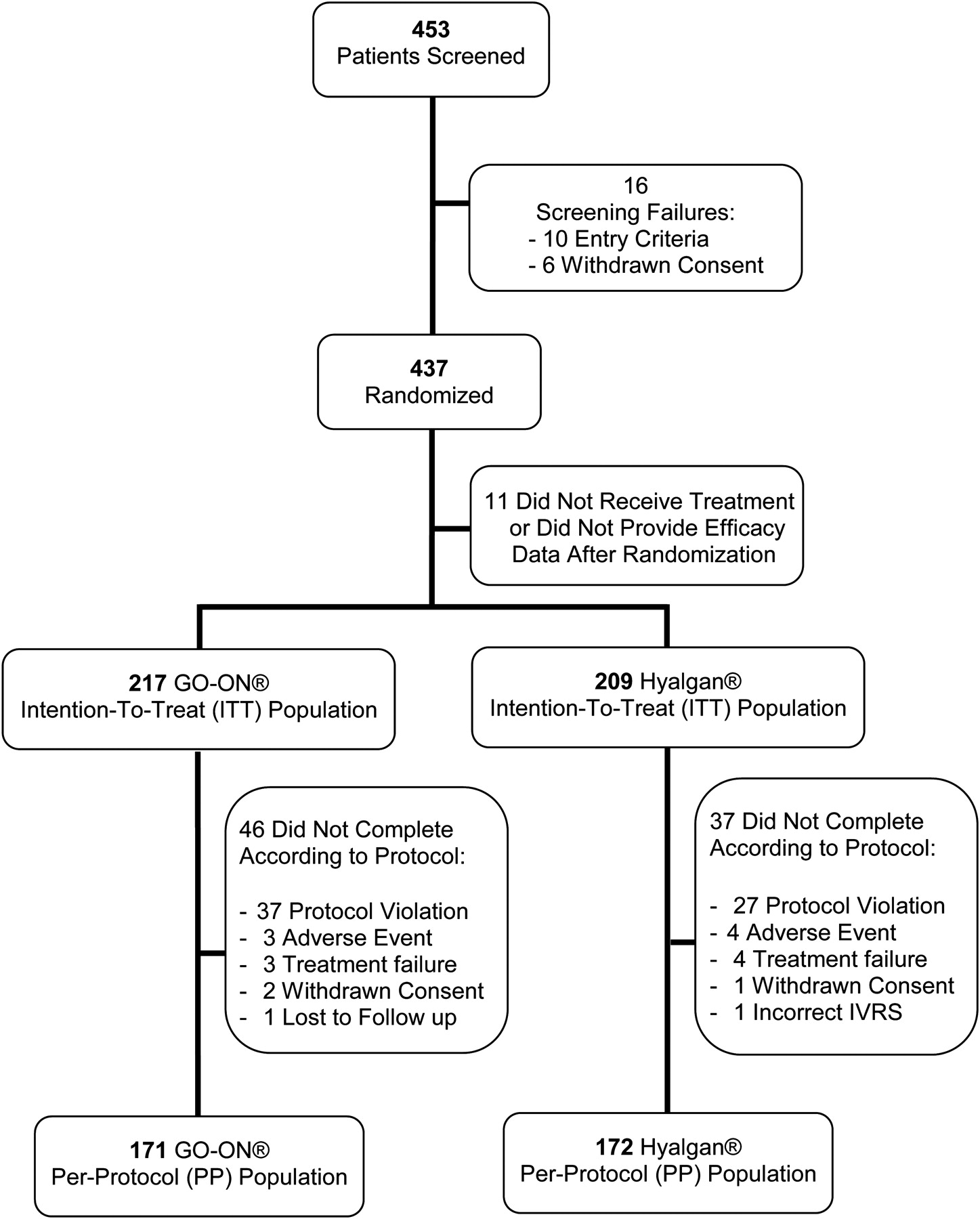
Patient disposition is described in figure 1. The first patient was enrolled in November 2008 and the last patient was completed in November 2009. Out of 437 patients randomly assigned, 217 and 209 in the GO-ON and Hyalgan groups, respectively, were included in the ITT population, thus excluding only 11 patients according to the predefined criteria. Protocol violations were the main reason for exclusion from the PP population, and consisted mainly of failure to meet the inclusion/exclusion criteria or use of prohibited medications. Less than 10% of patients were withdrawn for other reasons (AE, treatment failure, withdrawal of consent, other). All withdrawals/exclusions were similarly distributed between groups.

Trial profile.
Table 1 shows the demographic and baseline characteristics of the ITT population, without differences between groups and well representative of the common knee osteoarthritis outpatient population: mostly women (63%), mean age approximately 67 years, moderately overweight (average body mass index approximately 28) and with Kellgren and Lawrence radiological grades II and III evenly distributed. Knee osteoarthritis symptoms were moderate to severe, with average pain and function scores in the middle of their scales, pain VAS of the signal knee greater than 60 mm and Lequesne index approximately 11 points. There were no differences between the ITT and PP baseline populations (data not shown).
Patient demographic and baseline characteristics in the ITT population
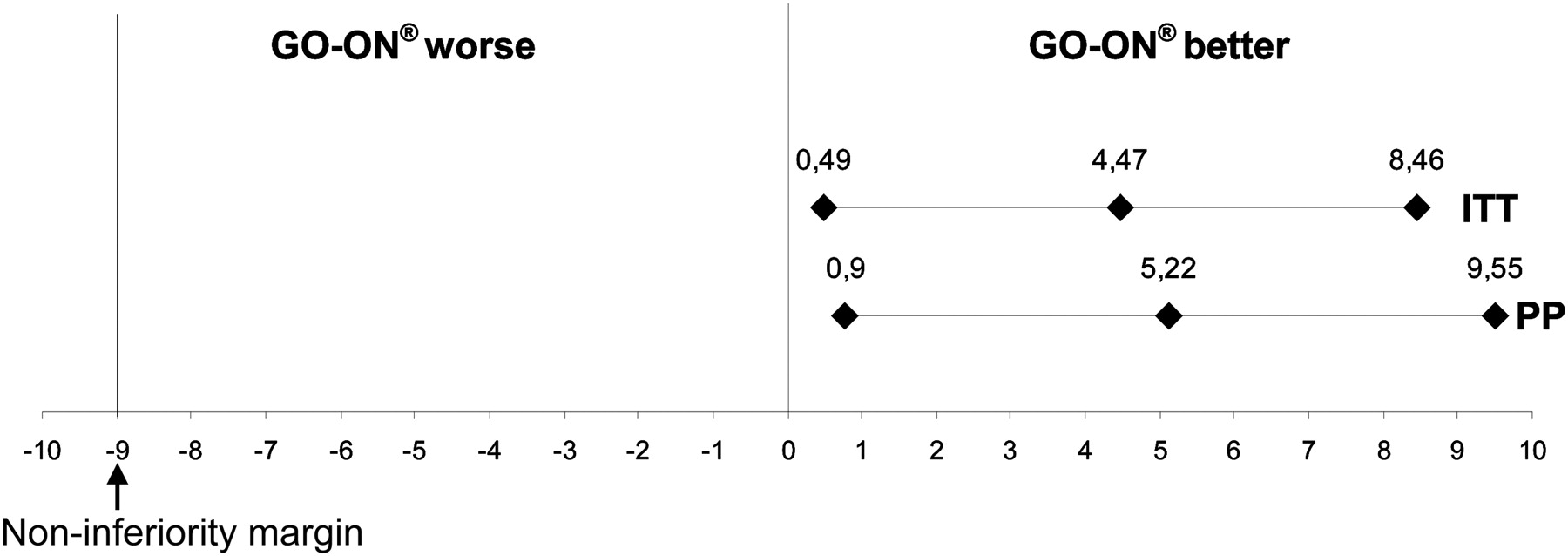
The ITT changes from baseline in the WOMAC pain subscale are reported in figure 2. Patients in both groups improved markedly during the first month after treatment and the effect was maintained for the duration of the study, with GO-ON exhibiting an overall better trend, that was particularly consistent between 12 and 24 weeks after the end of treatment. After 6 months from the end of treatment (ie, week 26), patients who had received GO-ON had decreased their WOMAC pain score by 22.9±1.4 mm (mean±SE), compared with 18.4±1.5 mm with Hyalgan in the ITT population. The primary analysis was first conducted on the PP population according to the non-inferiority study design and then on the ITT population. The changes from baseline and their 95% CI are reported in figure 3; as in both PP and ITT the lower limit of the 95% CI was higher than the predefined margin of −9 mm, this allowed us to conclude to the treatment non-inferiority. Furthermore, as this lower limit was above 0, the ITT analysis also allowed us to conclude to the statistical superiority of GO-ON versus Hyalgan (p=0.021) (figures 2 and 3, table 2), with an effect size of 0.21. This result did not change in a sensitivity analysis including the 11 patients excluded from the ITT population, according to a stricter ITT approach accounting for all randomly assigned patients (p=0.026).

Intention-to-treat mean (and SE) change from baseline at each assessment time point for the Western Ontario and McMaster Universities pain subscale score in the two groups receiving GO-ON (n=217) or Hyalgan (n=209). The arrows indicate the intra-articular injections.

{kind=link}
{kind=link}
{kind=link}
Point estimate and 95% CI of the difference (GO-ON vs Hyalgan, in mm) in the primary outcome represented by the Western Ontario and McMaster Universities pain subscale mean improvement. Values are differences in mean changes between GO-ON and Hyalgan at 6 months after treatment in the per-protocol (PP) and intention-to-treat (ITT) populations (−9 mm was the non-inferiority margin).
Mean changes (and 95% CI) from baseline to the endpoint (week 26, ie, 6 months after the end of treatment) in the ITT population for primary (WOMAC pain subscale) and secondary outcomes, including number (and percentages) of OARSI/OMERACT responders and of patients achieving MCII and PASS, with difference between groups and p value
Table 2 shows this superiority pattern for the majority of the secondary endpoints. Global knee pain VAS decreased by over 50% with GO-ON at week 26, but less with Hyalgan (effect size 0.26). A similar degree of efficacy was detected for all WOMAC scales and the Lequesne index underwent an over 4-point decrease with GO-ON versus 3 points with Hyalgan (effect size 0.34). The degree of improvement was similar for the ICOAP index, but the difference between groups was barely significant only for constant pain, while the two preparations behaved similarly on intermittent pain. Patients had also improved their global assessment VAS by almost 20 mm with GO-ON, but the better trend versus Hyalgan was not significant in ITT (p=0.068, table 2), but only in the PP analysis (p=0.044, data not shown).
Table 2 also shows that there were 73% OARSI/OMERACT responders 6 months after the end of treatment with GO-ON, versus 58% with Hyalgan (difference 14.9%, p=0.001). The proportion of patients achieving MCII and PASS for global knee pain, function and PGA was also high with both treatments but significantly higher with GO-ON than with Hyalgan except for global pain PASS and MCII for PGA (table 2).
All superiority trends were similar at the 12-week endpoint (data not shown), with a significant difference in the proportion of OARSI/OMERACT responders, 69.6% with GO-ON versus 60.3% with Hyalgan (p=0.044).
Patients used the rescue medication in a similar proportion: 166 out of 217 on GO-ON (77%) and 154 out of 209 (74%) with Hyalgan (p=0.50), with a low paracetamol daily mean consumption (218 and 223 mg/day, respectively, p=0.60); see supplementary text 3 (available online only).
The treatments were well tolerated. The proportion of patients reporting any AE in the safety population was similar: 74 out of 223 (33.2%) and 75 out of 213 (35.2%) with GO-ON and Hyalgan, respectively, most AE being unrelated to treatment. Back pain was the only AE reported with greater than 3% incidence. AE led to study discontinuation for three patients under GO-ON (worsening of knee osteoarthritis in two patients, only one of which was considered possibly related to the treatment, and one metastatic pulmonary cancer) and four patients under Hyalgan (worsening of knee osteoarthritis, post-traumatic meniscal lesion, ischaemic stroke, angiosarcoma with pleural effusion). Local AE are reported in table 3; both treatments were well tolerated locally. Although not statistically significant (p=0.17), the proportion of patients reporting local AE was double with Hyalgan (3.8%) compared with GO-ON (1.8%). No case of acute pseudoseptic arthritis was observed.
Number (and proportion) of patients with local AE at the injection site in the safety population
Discussion
In the present randomised, double-blind, controlled trial in over 400 knee osteoarthritis patients, three-weekly HA intra-articular injections decreased moderate to severe pain after 6 months by up to 50% of baseline values. Joint function improved to a similar extent and there were over 65% treatment responders on average with the two preparations used. The intermediate MW HA formulation GO-ON was not inferior to the reference low MW preparation Hyalgan on the WOMAC pain subscale score, but was also statistically superior on this primary and on most of the secondary outcomes as predetermined by the statistical analysis plan.12 ,13
While GO-ON tended to exhibit a trend for a better pattern of response throughout the study, both treatments behaved similarly well over the first month, when most of the therapeutic gain was observed, and during the first 3 months following the injection course. Afterwards, the benefit obtained with the low MW product tended to plateau, as acknowledged with most HA preparations,9 while there was a slight continuous improvement with GO-ON, ie, a more pronounced carry-over effect resulting in a statistically significant superiority on most outcomes after 6 months.
The primary endpoint was the change from baseline in the WOMAC pain subscale score, which displayed an extent of improvement similar to global knee pain VAS. The statistically significant ITT differences between treatments after 6 months were 4.5 and 6.4 mm, respectively, ie, below the minimum perceptible clinical improvement, usually set at approximately 10 mm22 and that was used to define the non-inferiority margin of 9 mm in this trial. Therefore, the clinical relevance of this statistical superiority is uncertain and it cannot be excluded that it is due to chance. However, the effect size ranged between 0.21 and 0.26 for the two pain endpoints, representing a small albeit clinically relevant difference. Moreover, there was a significantly higher proportion of OARSI/OMERACT responders after 6 months with GO-ON (73%) than with Hyalgan (58%), ie, a 15% difference that is beyond the accepted minimum clinically relevant improvement. The OARSI/OMERACT criteria require high improvement in pain or function (≥50% with absolute 0–100 change ≥20), or a moderate improvement (≥20% with ≥10 absolute change) in two out of pain, function or PGA, thus representing a real clinical improvement.18 Notably, there were significantly more OARSI/OMERACT responders with GO-ON already at the 12-week endpoint, as a prelude to the better carry-over effect that was then fully substantiated after 6 months. Similar proportions and differences in response rates were observed for patients reaching the MCII19 on pain and function after 6 months. Moreover, approximately 60% of patients achieved a PASS20 with GO-ON, with a significant difference compared with Hyalgan for function, but not for pain. PGA provided a slightly lower degree of improvement, without differences between treatments in absolute terms and as MCII, but with a more than 15% significantly higher proportion of patients reaching PASS with GO-ON.
A favourable feature of the present trial is that it assessed knee osteoarthritis symptoms through several different measures, providing a complete evaluation. Beside all WOMAC subscales showing a significant advantage for the intermediate MW product, the Lequesne index resulted in an effect size of 0.36 in favour of GO-ON. In addition, pain was also assessed by the new ICOAP index;17 interestingly, patients had slightly more severe baseline values for ‘intermittent’ pain, in which the two treatments displayed a similar efficacy, while GO-ON was better than Hyalgan on the slightly less severe ‘constant’ pain.
This study also has some limitations. First, there was no placebo comparison. This might have been an issue in the case of results limited to non-inferiority, given the debated efficacy of HA in general.9 However, as GO-ON was statistically superior to the low MW product and most of the differences were clinically relevant, this might represent sufficient evidence of efficacy. Moreover, ethics review boards might have raised ethical concerns in using intra-articular saline as a placebo when HA injections are now widely prescribed in knee osteoarthritis.
Second, it was not possible to provide identically appearing test and comparator preparations: the commercial preparations had to be used for obvious reasons, after appropriate packaging, and their effects may also differ given the different injected volumes. On the other hand, double-blind conditions were ensured by nominating at each site an ‘injector’ and a blinded ‘assessor’ investigator, while avoiding the patient's visual access to the injection field. Despite these difficulties, which are standard practice in these kind of trials, there was no evidence of broken double-blindness for any patient, reinforced by the strict assurance of adequately concealed random allocation by the interactive voice response system.
Third, this was a regulatory trial that was therefore industry-funded. Compared with non-industry-funded trials, sponsored studies more often yield results in support of the sponsor's drug.27 To avoid any potential allegations, an independent steering committee (FB, XC, FR, EM) supervised the trial design and study conduct, participated in blind data review meetings before database lock and provided binding recommendations for data management, finally accessing all results.
A fourth limitation was that the present trial only compared the intermediate HA product GO-ON with the reference low MW preparation, but not with a higher MW, cross-linked, formulation. While former studies suggested that high MW HA might have greater efficacy,4 in a recent meta-analysis11 showing that HA has more prolonged efficacy than intra-articular corticosteroids in knee osteoarthritis, five of the seven considered studies (and the only two high-quality trials) were performed with the low MW HA product used as reference in the present trial. Corticosteroids had a superior analgesic effect over the first 2 weeks, as expected, but from 8 weeks onwards and in particular 6 months after treatment HA had better pain control, with an effect size up to 0.39. Another meta-analysis10 found no evidence of a clinically relevant benefit of hylan compared with lower MW HA preparations, and a recent trial concluded to the non-inferiority between another intermediate MW HA and hylan G-F20.28 Actually, a study of single intra-articular hylan injection showed only a modest, albeit significant, benefit versus placebo over 6 months on knee pain, with less OARSI/OMERACT responders than with GO-ON in the present trial and a non-significant difference with placebo.29
A recent study has shown that low MW (50 000 Daltons) HA may have pro-inflammatory activity on chondrocytes, while intermediate MW preparations were neutral in this model of inflammation.30 It is difficult to transpose in-vitro results to humans and to the actual preparations used here, but this may partly explain the efficacy results of the present study, with good safety at the injection site compared with even higher MW products. Indeed, while in a recent trial hylan showed only a trend towards a higher incidence of local adverse reactions compared with placebo,29 previous studies suggested a doubling risk of local AE with the high MW HA preparation compared with lower MW products,10 which may be due to peptide contaminants, formaldehyde, or crystal-induced inflammation. In the present study, GO-ON and Hyalgan were equally well tolerated at the injection site, although numerically more local reactions occurred with Hyalgan than with GO-ON, therefore showing a very good safety of the latter.
In conclusion, this trial shows that the intermediate MW HA preparation GO-ON is effective on knee osteoarthritis symptoms over 6 months after a 3-weekly injection course, and may be more effective than the reference low MW formulation. Further studies are warranted to elucidate the mechanism of this possible superiority and more pronounced carry-over effect and to test whether this selected HA preparation has a prominent therapeutic profile compared with other HA products.
Acknowledgments
The authors wish to thank all the clinical investigators who took part in the conduct of this trial and provided and cared for study patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Funding This was a trial conducted for regulatory purposes and therefore received full financial support from the sponsor Rottapharm|Madaus. Co-authors SC, MD, GG and LCR are scientists from the Department of Clinical Pharmacology of Rottapharm|Madaus and agreed individually to be listed as co-authors due to their involvement in the study; there was no other involvement of the sponsor as a corporate entity in the conduct of the study and in the manuscript submission process. Co-authors FB and JG were the study principal investigators and received research grants for this. Co-authors FB, XC, FR and EM received a reimbursement fee for their involvement in the steering committee of the study.
-
Competing interests Rottapharm|Madaus is the sponsor of the study and the manufacturer of one of the preparations tested in this study (GO-ON) and has this preparation on the market in different countries of the world. The full trial protocol, all study documents including completed case record forms and the complete statistical database are available from the sponsor's good clinical practice archives.
-
Ethics approval Ethics approval was provided by the Comité de Protection des Personnes, AP-HP St-Antoine Hospital, Paris and the ethics committee of Regensburg University and by all applicable local ethics committees.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.